Androgenetic Alopecia: Causes, Symptoms, & Treatments – A Complete Guide
Executive Summary: Key Takeaways on Pattern Hair Loss
Androgenetic Alopecia, commonly known as pattern baldness, is the most frequent cause of hair loss globally. It affects millions of individuals, causing distress and a search for effective solutions. Understanding this condition is the first step toward managing it successfully. Here’s what you need to know:
- Root Cause: The primary driver is a genetic predisposition combined with the action of the androgen hormone, Dihydrotestosterone (DHT), which shrinks hair follicles.
- Key Treatments: The main, medically-proven interventions are oral Finasteride, topical Minoxidil, and Hair Transplantation (FUE/DHI). Newer methods like PRP and advanced topical serums also offer support.
- Proactive Management: Early diagnosis is crucial. Consulting a specialist early can preserve more hair and increase the success rate of treatments.
- Advanced Options: Modern hair transplant techniques, such as FUE and DHI, offer natural and long-lasting results for those seeking permanent restoration. You can read more about techniques here.
Hair loss, specifically Androgenetic Alopecia, can be a deeply personal and frustrating experience. It’s far more than just a cosmetic issue; it affects self-esteem, confidence, and overall quality of life. This comprehensive guide aims to demystify this common condition, offering authoritative, empathetic, and easy-to-understand insights into its origins, how to spot it, and, most importantly, the most effective modern treatments available today. Whether you’re an individual noticing the early signs or a professional seeking the latest clinical data, this article provides the clarity you need.
Moreover, modern medicine offers a range of sophisticated solutions, from non-surgical therapies to advanced hair restoration procedures. For those considering an international option, you might find our guide on the best country for hair transplant useful.
What is Androgenetic Alopecia? The Foundation of Pattern Hair Loss
In essence, Androgenetic Alopecia is a progressive, patterned form of hair loss, meaning it follows a predictable pattern. It affects a significant portion of the global population, including individuals who experience the patterns known as Male Pattern Baldness (MPB) (typically affecting up to 70% of those assigned male at birth) and Female Pattern Hair Loss (FPHL) (typically affecting up to 40% of those assigned female at birth) at some point in their lives. The term itself is a combination of two root words: “Androgenetic”, which refers to androgens (male hormones) and genetics, and “Alopecia”, which is simply the medical term for hair loss. It is a chronic condition driven by internal biological factors.
The Key Difference: MPB vs. FPHL Patterns
While the underlying cause—genetics and hormones—is similar, the presentation differs significantly:
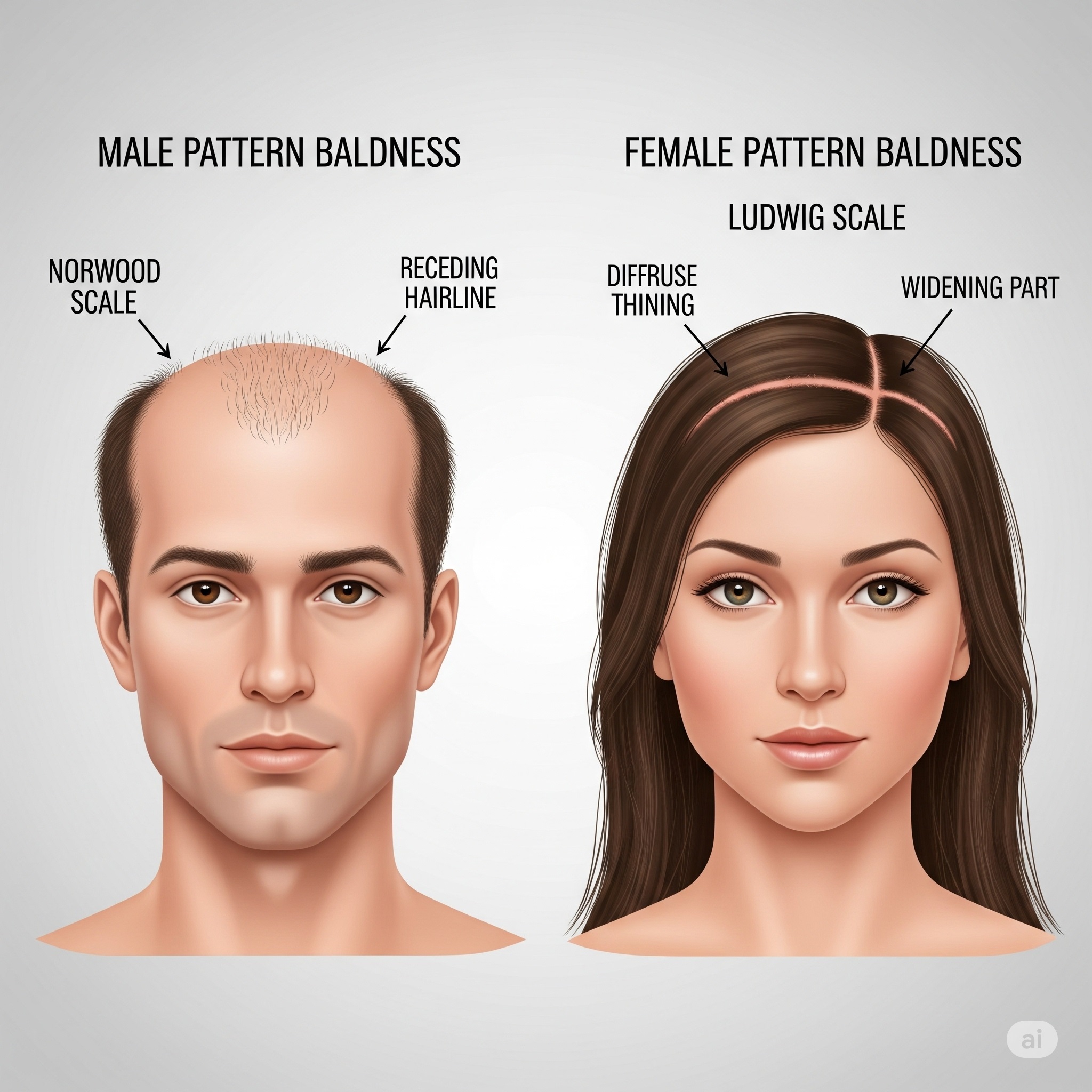
- MPB (The Male Pattern): Typically begins with a receding hairline and thinning at the crown, eventually leading to the classic ‘M’ or ‘U’ shape. It is classified using the Norwood scale.
- FPHL (The Female Pattern): Generally presents as a widening of the part, with diffuse thinning over the top of the scalp. The front hairline usually remains intact. It is classified using the Ludwig scale.
It’s important to acknowledge that this condition is extremely common and absolutely treatable, especially when caught early. You can find out more about understanding hair terms in our complete glossary.
Causes: The DHT Connection and Genetic Blueprint
The core mechanism of Androgenetic Alopecia is a multi-factor issue, but two elements stand out: hormones and heredity. Interestingly, recent studies are also exploring other environmental co-factors that may influence the progression of this condition, though the genetic and hormonal link remains paramount.
The Role of Dihydrotestosterone (DHT)
This is arguably the most critical piece of the puzzle. Testosterone, a powerful androgen, converts into **Dihydrotestosterone (DHT)** through an enzyme called **5-alpha reductase**. For individuals genetically predisposed to pattern hair loss, the hair follicles on the scalp are highly sensitive to DHT. When DHT binds to receptors on these follicles, it triggers a process called **follicular miniaturization**.
This miniaturization cycle leads to:
- The hair’s growth phase (Anagen) shortens significantly.
- The hair shaft becomes progressively thinner, shorter, and lighter in color.
- Eventually, the follicle shrinks so much that it can no longer produce visible hair.
Therefore, managing DHT is a key strategy in treating Androgenetic Alopecia.
Genetic Predisposition
It’s a common misconception that hair loss only comes from the mother’s side of the family. While the X chromosome (inherited from the mother) plays a significant role, research shows that multiple genes on different chromosomes contribute to a person’s likelihood of developing pattern baldness. Consequently, if hair loss is common on either side of your family, your risk is elevated. Genes control the number of androgen receptors in the hair follicles, thus determining their sensitivity to DHT.
Symptoms and Diagnosis: Recognizing the Early Signs
Recognizing the symptoms early is vital because treatment is far more effective at preventing further loss than regrowing lost hair. Don’t wait until the pattern is severe to seek help.
Identifying the Signs of MPB and FPHL
While the overall result is hair loss, the path there is distinct:
- For Individuals with MPB: The first noticeable sign is often a receding hairline, particularly at the temples. This is followed by thinning on the crown (vertex). The two areas gradually merge.
- For Individuals with FPHL: Those experiencing this pattern rarely go completely bald. The hallmark is a diffuse thinning on the top of the scalp. You may notice your central hair part gradually becoming wider, or your ponytail feels less substantial.
The Diagnostic Process
A diagnosis of Androgenetic Alopecia is usually straightforward and typically involves:
- Clinical Examination: A dermatologist or hair specialist examines your scalp pattern, often using a magnifying tool like a dermatoscope to check for miniaturized hairs.
- Medical History: The doctor reviews your family history and any related health issues, especially thyroid or hormonal imbalances.
- Blood Tests: Sometimes, tests are ordered to rule out other causes of hair loss, such as iron deficiency, thyroid disease, or autoimmune conditions.
Who is This For? Understanding Candidacy
This information is vital for anyone experiencing or worried about hair thinning. Knowing your current stage helps determine the best treatment path:
- Individuals with Early-Stage Hair Loss (Norwood 1-3, Ludwig I): You are the best candidate for non-surgical medical therapies to stabilize and potentially regrow hair. Proactive intervention here is key.
- Individuals with Moderate to Advanced Hair Loss (Norwood 3-5, Ludwig II-III): You are likely a candidate for a combination approach—medical therapy to prevent further loss and hair transplantation to restore density to bald or severely thinned areas.
- Anyone Seeking Permanent Restoration: If you have a stable donor area and realistic expectations, hair transplant surgery offers the most permanent solution to pattern baldness. Learn more about one procedure here.
Treatments: A Detailed Breakdown of Medical and Surgical Options
The landscape of Androgenetic Alopecia treatment has never been more promising. The most effective strategies utilize a dual approach: medication to halt progression and surgery to restore lost density.
Pharmaceutical Treatments (Non-Surgical)
These are the foundation of any treatment plan for pattern hair loss.
Finasteride (Oral)
Finasteride is a prescription oral medication that works by blocking the 5-alpha reductase enzyme, thereby significantly lowering DHT levels in the scalp and blood. This action slows or stops the miniaturization process and can even lead to regrowth in some cases.
- Highly effective at halting hair loss progression, often more so than Minoxidil.
- Simple to take (one pill daily).
- Targets the root hormonal cause (DHT).
- Requires a prescription and ongoing use.
- Potential, though rare, side effects include sexual dysfunction.
- Primarily approved for the treatment of **Androgenetic Alopecia** in individuals assigned male at birth.
Minoxidil (Topical or Oral)
Minoxidil is an over-the-counter treatment applied directly to the scalp or, increasingly, taken in a low-dose oral format. It is a vasodilator, meaning it widens blood vessels, which is thought to increase blood flow to the follicles, delivering more nutrients. It also extends the anagen (growth) phase of the hair cycle.
- Available without a prescription.
- Effective for individuals of all genders (with concentrations usually differing based on typical pattern use, such as 5% for the male pattern and 2% for the female pattern).
- Generally safe with minimal systemic side effects.
- Requires twice-daily application (for topical) which can be messy.
- Effectiveness stops if use is discontinued.
- Can sometimes cause scalp irritation or dryness.
Advanced Surgical Treatments (Hair Transplantation)
For areas where miniaturization has progressed to complete baldness, transplantation offers a permanent solution by moving DHT-resistant follicles from the back and sides of the scalp to the thinning areas.
Follicular Unit Extraction (FUE)
FUE is the most popular modern technique. It involves individually extracting follicular units (naturally occurring groups of 1-4 hairs) from the donor area using a small punch tool, creating tiny, unnoticeable scars. These units are then implanted into recipient sites.
- Minimal scarring (tiny dots that are easily concealed even with short hair).
- Faster recovery time compared to older methods.
- Allows for precise placement and a highly natural result. You can see cost information here.
- Requires shaving the donor area.
- Can be time-consuming for large sessions.
- Generally more expensive per graft than the FUT method.
Direct Hair Implantation (DHI)
DHI is a modification of FUE where a specialized implanter pen (like a Choi Pen) is used to both create the recipient site and place the graft simultaneously. This technique is known for its high-density results and minimal trauma to the grafts.
- Allows for maximum density and a highly natural look.
- Often enables transplantation without fully shaving the recipient area.
- Improved graft survival rates due to reduced out-of-body time.
- Requires highly specialized and skilled surgeons.
- Can be more expensive than standard FUE.
- Only suitable for certain hair characteristics.
For those considering the surgical route, it’s essential to research reputable clinics and surgeons. You can check out our guide to Best Hair Transplant Clinics in Turkey.
Supplemental and Emerging Therapies
While not primary treatments for Androgenetic Alopecia, these therapies are often used in combination with medication or surgery to boost results and improve scalp health.
Platelet-Rich Plasma (PRP) Therapy
PRP involves drawing a small amount of the patient’s blood, processing it to concentrate the platelets (which contain growth factors), and injecting the resulting plasma into the scalp. These growth factors stimulate dormant hair follicles and promote healing.
- Uses the body’s own resources, minimizing allergic reactions.
- Can boost the thickness and health of existing, miniaturized hairs.
- Excellent adjunctive therapy post-transplant.
- Efficacy can vary widely between patients and clinics.
- Requires multiple sessions (typically 3-4 initial, then maintenance).
- Still considered an “off-label” treatment by some regulatory bodies.
Low-Level Laser Therapy (LLLT)
LLLT uses devices (combs, caps, or helmets) to deliver red light energy directly to the scalp. This energy is thought to be absorbed by hair follicles, stimulating cell metabolism and encouraging hair growth. It can be a convenient at-home treatment.
- Non-invasive and easy to use at home.
- FDA-cleared for treating pattern baldness.
- No known systemic side effects.
- Results are modest and take several months of consistent use to appear.
- Devices can be expensive.
- Effectiveness is not as potent as Finasteride or Minoxidil.
Comparison Table: Primary Treatment Options for Androgenetic Alopecia
Choosing the right approach can be difficult, so we’ve compiled a quick comparison of the three primary treatments:
| Treatment | Mechanism | Target | Permanence |
|---|---|---|---|
| Finasteride (Oral) | Blocks DHT conversion (Hormonal Blocker) | Halting further miniaturization/loss | Temporary (Must be used continuously) |
| Minoxidil (Topical/Oral) | Increases blood flow; prolongs growth phase | Stimulating existing, miniaturized follicles | Temporary (Must be used continuously) |
| Hair Transplant (FUE/DHI) | Moves DHT-resistant follicles to bald areas | Restoring density to bald or thin areas | Permanent (For the relocated hair) |
Case Study: John’s Journey with Androgenetic Alopecia
Patient Profile: John, a 35-year-old marketing manager, noticed significant thinning in his temples and crown over three years. He was classified as a Norwood Scale III vertex (Male Pattern Baldness), with hair loss impacting his confidence during client meetings. His father and maternal grandfather both experienced pattern baldness.
Diagnosis & Initial Treatment: After a trichoscopy confirmed active miniaturization, John was diagnosed with Androgenetic Alopecia. His doctor recommended a dual non-surgical approach:
- Finasteride (1mg daily): To stabilize the hormonal cause and prevent further loss.
- Topical Minoxidil (5% twice daily): To stimulate existing, thinning hair on the crown.
Outcome after 12 Months: John’s hair loss stabilized completely. His crown showed notable thickening, but the deeply receded temples had minimal regrowth. The existing thinning hairs improved, but the bald patches remained. For better results, he explored options for a hair transplant abroad.
Next Step (Advanced Treatment): He opted for a targeted FUE hair transplant, focusing 2,500 grafts on restoring his hairline and filling the recessed temples. He maintained his Finasteride and Minoxidil regimen.
Final Result (18 Months Post-Surgery): John achieved a dense, natural-looking hairline and full coverage in his temples. He continues the medication to protect his remaining native hair. His case illustrates the power of combining medical stabilization with surgical restoration for optimal results in combating Androgenetic Alopecia.
Frequently Asked Questions (FAQ) About Androgenetic Alopecia
1. Is Androgenetic Alopecia curable?
No, it is a chronic, progressive condition rooted in genetics. However, it is highly treatable. Medications can effectively halt or slow the progression, and hair transplantation offers a permanent restorative solution for lost hair.
2. Does stress cause Androgenetic Alopecia?
While severe stress can trigger a temporary shedding condition called Telogen Effluvium, it does not directly cause the genetic and hormonal hair loss of Androgenetic Alopecia. Stress, however, can potentially accelerate or exacerbate existing pattern baldness.
3. How long does it take to see results from Finasteride or Minoxidil?
You must be patient. It typically takes 4 to 6 months of consistent use to see noticeable stabilization or regrowth, and full results are usually assessed at 12 months. Stopping treatment will cause the benefits to reverse within a few months.
4. Can individuals assigned female at birth take Finasteride?
Finasteride is generally not prescribed to premenopausal individuals assigned female at birth due to the risk of birth defects in male fetuses. It may be used cautiously and sometimes off-label in postmenopausal individuals who have not responded to other treatments, but its primary use is for the male pattern of the condition.
5. What is “shock loss” after a hair transplant?
Shock loss is a temporary shedding of existing native hairs (not the transplanted grafts) that can occur a few weeks after a hair transplant due to the trauma of the surgery. It almost always regrows within a few months. Read more about hair transplant side effects here.
6. Is a hair transplant really permanent?
Yes. The transplanted hairs are taken from the donor area (back and sides of the head), which are genetically resistant to the effects of DHT. When moved, they retain this resistance, making the result permanent. You can learn more about long-term results here.
7. What is the minimum age for a hair transplant?
Most reputable surgeons prefer patients to be over 25, or at least have a stable pattern of hair loss, to ensure the procedure is done correctly and accounts for future loss. Early transplantation risks an unnatural-looking pattern as surrounding hair continues to thin.
8. Do I need to continue medication after a hair transplant?
Yes, most specialists strongly recommend continuing Finasteride and/or Minoxidil. While the transplanted hairs are safe, the surrounding native hairs are still susceptible to Androgenetic Alopecia and will continue to thin without medical intervention.
9. Are there any natural remedies for pattern baldness?
While some supplements like biotin or saw palmetto are promoted, none have the proven, robust clinical data to rival Finasteride or Minoxidil. They may be used as adjunctive support but should not replace proven medical treatment for Androgenetic Alopecia.
10. Can iron deficiency mimic FPHL in individuals?
Yes, it can. Low ferritin (iron stores) is a common cause of diffuse hair shedding in individuals. This is why a thorough blood test is often part of the diagnostic process to distinguish it from FPHL or to treat both conditions simultaneously.
11. What is the difference between FUE and DHI?
Both are forms of modern hair transplant. FUE involves a two-step process (extraction, then incision/implantation). DHI is a one-step implantation using a specialized tool (Choi pen) that simultaneously creates the site and places the graft, often allowing for higher density and less trauma.
12. Is hair loss from Androgenetic Alopecia irreversible without surgery?
Follicular miniaturization is reversible with medication (Finasteride/Minoxidil) only if the follicle is still alive, producing thin vellus hair. If the follicle has completely shrunk and scarred over, only a hair transplant can restore hair to that area.
13. Where can I find top-rated hair transplant specialists?
Expertise is global. Many patients seek advanced, cost-effective care abroad. You can find information on top clinics in destinations like Turkey via our resource on Top Hair Transplant Doctors in Istanbul.
14. Is it possible to have hair thinning without a receding hairline?
Yes, especially in the early stages of MPB (vertex thinning) or in FPHL, where the hairline is typically preserved, and thinning occurs as a widening of the central part.
15. What are the key things to consider when choosing a hair transplant clinic?
Focus on the surgeon’s experience, the technique used (FUE or DHI), patient testimonials and verifiable before/after photos, and the all-inclusive cost, including aftercare. For cost transparency, check out our guide on Hair Transplant Cost in Istanbul.
Credibility and Expert Insights
The management of Androgenetic Alopecia is continually evolving. Recent research has focused heavily on genetics and better understanding the inflammatory component of the condition. For example, recent findings highlight the importance of the Prostaglandin D2 (PGD2) pathway as an inhibitor of hair growth, opening new avenues for future drug development beyond DHT blockage. Furthermore, the rising success of low-dose oral Minoxidil has offered a less irritating alternative to topical application, increasing patient compliance significantly according to recent dermatological reviews.
Additionally, while Finasteride is highly effective, the conversation around side effects is critical. Authoritative sources like the Mayo Clinic continue to emphasize that for the vast majority of individuals, the benefits of hair retention far outweigh the small, reversible risk of side effects. Always have an open, honest discussion with a certified physician.
Final Thoughts and Taking Action
Living with Androgenetic Alopecia doesn’t mean passively accepting hair loss. It means engaging in an active, informed, and proactive management plan. From daily medication to advanced surgical techniques, effective solutions exist to help you retain, restore, and improve your hair density. The most important step is consulting a specialist early to tailor a treatment regimen to your specific needs and hair loss stage. Remember, the journey to restoration often involves multiple steps, including sometimes exploring options like a hair transplant in Turkey for quality care and cost efficiency.
Learn more about your options, consult with experts, and take control of your hair loss today. The future of hair restoration is here, and it’s customized for you.
Start Your Hair Restoration Journey Today: Contact Us
External Resources and Further Reading
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS)
- Harvard Health Publishing
- Cardiac Surgery Department
- Gynecological Surgery Department
- Orthopedic Surgery Department
- Plastic Surgery Department
- Lung and Thoracic Surgery Department
- Skin and Hair Department
- Dental Department
- Neurosurgery Department
- Urological Surgery Department
- ENT Surgery Department
- Oncology Department
- Checkup Department
- General Surgery Department
- Ophthalmology Department
- Find an Expert Doctor



