❤️ Compare TAVI and Open-Heart Surgery: A Comprehensive Guide for 2026 🏥
Facing a heart condition involves making critical decisions. When your doctor mentions aortic stenosis, the next conversation usually revolves around treatment options. This guide will help you compare TAVI and open-heart surgery (SAVR) to empower your healthcare journey.
Executive Summary: Key Takeaways
Before we dive deep, here is a quick overview for those in a hurry. When we compare TAVI and open-heart surgery, we look at invasiveness, recovery, and durability.
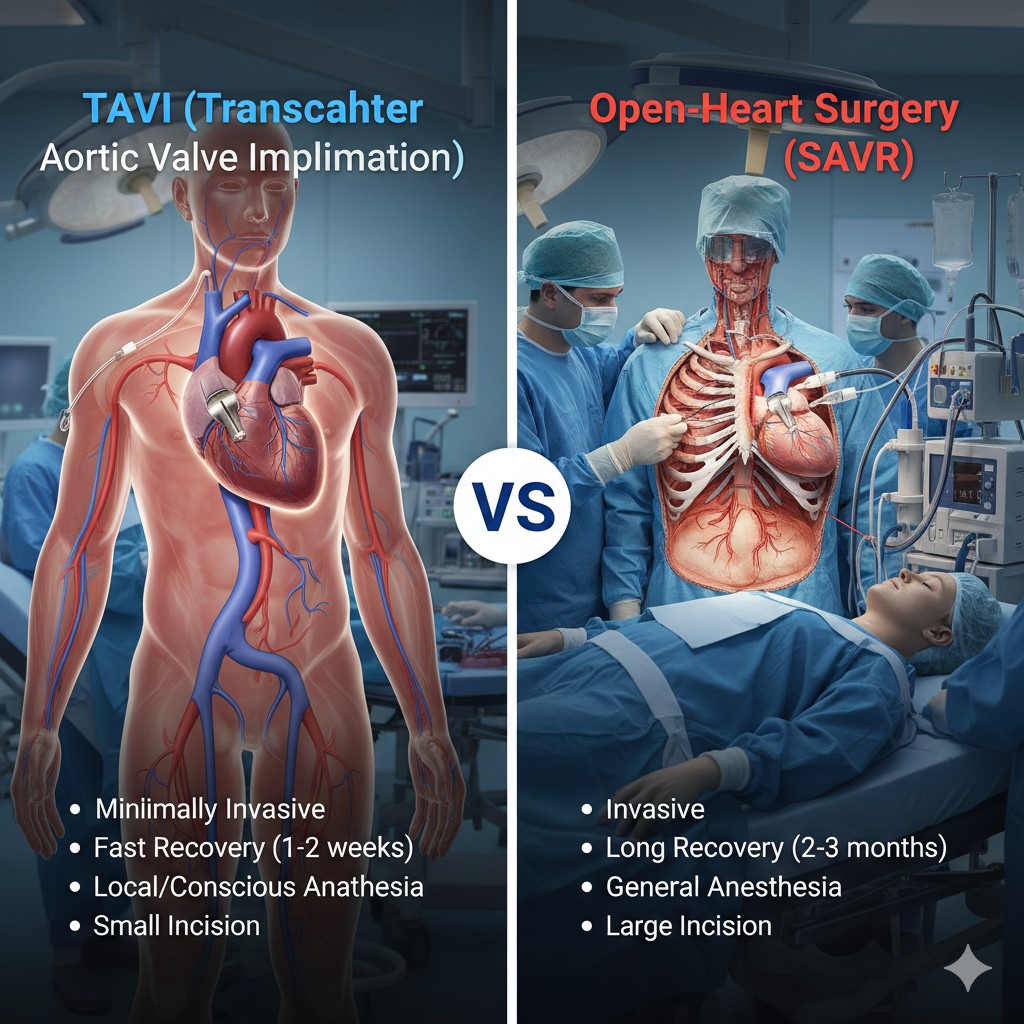
- Invasiveness: TAVI is minimally invasive (catheter-based), while open-heart surgery requires a chest incision.
- Recovery: TAVI patients often walk within 24 hours. Surgery requires weeks of healing.
- Cost: Medical tourism destinations offer both at significantly reduced rates compared to the West.
- Suitability: Surgery is often preferred for younger patients; TAVI is favored for older or high-risk patients.
Understanding the Basics: What Are We Comparing?
Your heart has four valves. The aortic valve controls blood flow from the heart to the rest of the body. Over time, this valve can narrow, a condition called aortic stenosis. Consequently, the heart works harder, leading to fatigue and chest pain. To fix this, we must replace the valve.
What is Open-Heart Surgery (SAVR)?
Surgical Aortic Valve Replacement (SAVR) is the traditional gold standard. A cardiac surgeon makes an incision in the chest to access the heart directly. The heart is temporarily stopped. A heart-lung machine takes over blood circulation. Then, the surgeon removes the damaged valve and sews in a new one.
What is TAVI (Transcatheter Aortic Valve Implantation)?
TAVI, sometimes called TAVR, is a modern alternative. It stands for Transcatheter Aortic Valve Implantation. Instead of opening the chest, doctors insert a catheter into an artery, usually in the groin. They guide a collapsible valve through the tube to the heart. Once in place, the new valve expands and pushes the old valve leaflets aside. The heart continues to beat during this procedure.
You can learn more about valve procedures in our valve repair and replacement section.
Deep Dive: Open-Heart Valve Replacement (SAVR)
For decades, SAVR has saved countless lives. It remains a robust solution, particularly for specific patient groups. Let’s break down the advantages and disadvantages.
The Advantages of SAVR
Proven Durability: We have decades of data on surgical valves. We know they last. For a patient in their 50s, this long-term data provides peace of mind.
Correction of Other Issues: During open surgery, surgeons can fix other problems simultaneously. For example, if you need Coronary Artery Bypass Grafting (CABG) or aortic root repair, doing it all at once is logical.
Precise Sizing: With direct vision, surgeons can size the valve perfectly and remove calcium deposits that might interfere with placement. This reduces the risk of leaks around the new valve.
The Disadvantages of SAVR
Trauma and Recovery: The sternotomy (breastbone incision) is traumatic. The bone takes 6 to 8 weeks to heal. Patients cannot drive or lift heavy objects during this time. Pain management is a significant part of the early recovery phase.
Infection Risk: Larger incisions inherently carry a higher risk of wound infection compared to a needle puncture. However, prophylactic antibiotics minimize this.
Anesthesia Requirements: General anesthesia is mandatory. For older patients or those with cognitive decline, prolonged anesthesia can have side effects.
Deep Dive: TAVI (Transcatheter Aortic Valve Implantation)
TAVI has revolutionized cardiology. Originally reserved for patients too sick for surgery, it is now an option for many low-risk patients. When you compare TAVI and open-heart surgery, TAVI shines in patient comfort.
The Advantages of TAVI
Minimally Invasive: There is no broken bone. The entry point is a small puncture in the femoral artery. Consequently, there is minimal scarring.
Rapid Recovery: This is the biggest selling point. Many patients go home the next day. You can return to normal activities within a week. For older adults, preserving independence is crucial.
Less Pain: Post-procedural pain is significantly lower. Most patients only require mild pain relievers, avoiding strong opioids.
Conscious Sedation: TAVI often does not require general anesthesia. You might be awake but sedated. This reduces grogginess and complications related to breathing tubes.
The Disadvantages of TAVI
Vascular Complications: Because large catheters travel through arteries, there is a risk of damaging the blood vessel. However, smaller modern devices have reduced this risk.
Pacemaker Requirement: The electrical system of the heart sits near the aortic valve. The pressure from the TAVI valve can sometimes disrupt this, requiring a permanent pacemaker. This happens more often with TAVI than with SAVR.
Paravalvular Leak: Sometimes, the valve doesn’t seal perfectly against the calcium of the old valve. This allows small amounts of blood to leak backward. Newer valve designs have skirts to prevent this.
If you are considering this procedure, a consultation is vital. You can book a telemedicine consultation with our experts to discuss your anatomy.
Head-to-Head: Compare TAVI and Open-Heart Surgery
The table below provides a direct comparison to help you visualize the differences.
| Feature | Open-Heart Surgery (SAVR) | TAVI / TAVR |
|---|---|---|
| Incision | Large chest incision (Sternotomy) | Small puncture (usually groin) |
| Anesthesia | General Anesthesia (Mandatory) | General or Conscious Sedation |
| Hospital Stay | 5 to 7 days | 1 to 3 days |
| Recovery to Normal Life | 2 to 3 months | 1 to 2 weeks |
| Pain Level | Moderate to High (initial weeks) | Minimal |
| Durability | Proven (15+ years for tissue) | Promising (Good 5-8 year data) |
| Pacemaker Risk | Lower | Higher |
Who is This For? Choosing the Right Path
Not everyone is a candidate for TAVI, and not everyone should have open surgery. Doctors use risk stratification to decide. They compare TAVI and open-heart surgery based on your specific health profile.
High-Risk and Older Patients
If you are over 75 or have other conditions like kidney disease or weak lungs, open surgery is risky. TAVI is almost certainly the better choice here. The body handles the catheter procedure much better than the trauma of surgery.
Intermediate-Risk Patients
Recent trials show TAVI is as good as surgery for this group. The choice often comes down to anatomy. If your arteries are too small for the catheter, surgery might be safer.
Low-Risk and Younger Patients
This is where the debate is active. For patients under 65, surgery is often recommended. Why? Because we need the valve to last 20 years. If a TAVI valve fails in 10 years, putting a second one in is harder. A surgical valve sets a strong foundation. Additionally, mechanical valves (which last forever but require blood thinners) are only available via surgery.
For a detailed assessment, you can visit our clinics in Iran or check our facilities in Mashhad.
Case Study: The Journey of Two Hearts
Let’s look at two hypothetical patients to illustrate the decision process.
Patient A: Robert (78 Years Old)
Robert enjoys gardening but has felt dizzy lately. He has mild COPD (lung issues) from smoking years ago. His diagnostic tests show severe aortic stenosis.
The Decision: His medical team decides to compare TAVI and open-heart surgery. Because of his age and lung condition, open surgery carries a high risk of pneumonia during recovery. Robert chooses TAVI.
The Outcome: He undergoes the procedure on a Tuesday. By Wednesday afternoon, he is sitting in a chair. He goes home on Thursday. Two weeks later, he is back in his garden. His recovery was seamless.
Patient B: Sarah (55 Years Old)
Sarah is an active teacher. She was born with a bicuspid aortic valve (a congenital defect) that has now calcified. She is otherwise very healthy.
The Decision: The heart team discusses options. Sarah wants a solution that lasts as long as possible. TAVI is technically possible, but her bicuspid anatomy makes it tricky. Furthermore, she is young.
The Outcome: Sarah chooses open-heart surgery. She receives a high-quality tissue valve. Her recovery takes 8 weeks, which is tough, but she heals well. She likely won’t need another intervention for 15 to 20 years.
Whether you are like Robert or Sarah, we can help. Explore our comprehensive health checkups to start your assessment.
The Patient Roadmap: Your Steps to a New Heart
Navigating cardiac care abroad can seem daunting. Here is a roadmap to simplify the process.
Step 1: Diagnosis and Records
You need an echocardiogram and an angiogram. Gather your medical reports. You can upload these for a remote review via our contact page.
Step 2: The Consultation
Our specialists will review your files. They will compare TAVI and open-heart surgery specifically for your anatomy. We will provide a treatment plan and a cost estimate.
Step 3: Travel and Preparation
We assist with visas, flights, and accommodation. Upon arrival, you will undergo pre-operative anesthesia consultation to ensure safety.
Step 4: The Procedure
Whether it is TAVI or surgery, our partner hospitals use state-of-the-art technology. You are in safe hands.
Step 5: Recovery and Return
For TAVI, you might enjoy a bit of tourism in the city after a few days. For surgery, you will rest in a medical hotel until fit to fly.
Cost Analysis and Medical Tourism
Cost is a massive factor. In the US, TAVI can cost over $50,000 to $80,000. Open heart surgery is similarly expensive. However, medical tourism changes the equation.
Why Choose WMedTour?
We connect you with JCI-accredited hospitals in affordable destinations. By choosing to travel, you can save up to 70% without compromising quality.
- Turkey: Known for excellent hospitality and advanced European-standard cardiac centers. See our Turkey tours.
- India: Home to some of the world’s most skilled high-volume surgeons. Check our India medical packages.
- Iran: Offers incredibly competitive pricing for high-level surgical expertise. Explore Iran options.
Below is a general cost comparison (estimates):
| Procedure | USA / UK Cost (Approx) | Medical Tourism Cost (Approx Start) |
|---|---|---|
| TAVI | $60,000+ | $18,000 – $25,000 |
| Open Heart (SAVR) | $50,000+ | $8,000 – $15,000 |
Note: Prices vary by valve type and hospital choice.
Recovery and Lifestyle
When you compare TAVI and open-heart surgery, the recovery phase is where they differ most. However, the long-term goal is the same: a healthy life.
Cardiac Rehab
Regardless of the method, cardiac rehabilitation is recommended. It strengthens your heart safely. We can arrange initial rehab sessions before you fly home.
Diet and Medication
You may need blood thinners for a short period. A heart-healthy diet is essential. We offer cardiac checkups to monitor your progress annually.
Conclusion: Making the Choice
To compare TAVI and open-heart surgery is to balance immediate recovery against proven long-term data. TAVI offers a quick return to life, perfect for the olders. Open surgery offers a durable reconstruction, ideal for the young.
Your heart is unique. Your treatment should be too. If you are ready to explore your options or need a second opinion, contact WMedTour today. We are here to guide you to the best hospitals worldwide.
For more insights, read our about us page or browse our articles.
Frequently Asked Questions
What is the main difference between TAVI and open-heart surgery?
The main difference lies in invasiveness. Open-heart surgery (SAVR) requires a large incision and stopping the heart. Conversely, TAVI is minimally invasive, using a catheter through an artery, usually in the groin, to place the valve while the heart beats.
Is TAVI safer than open-heart surgery for older patients?
Generally, yes. TAVI is often safer for older patients or those with high surgical risks. It avoids the physical trauma of opening the chest and the need for a heart-lung machine, leading to faster initial recovery.
How long does the TAVI valve last compared to a surgical valve?
Surgical tissue valves have a long track record, lasting 10–20 years. TAVI data is newer but promising, showing similar durability over 5–8 years. Long-term data beyond 10 years for TAVI is still being gathered.
Can I travel for TAVI or open-heart surgery?
Yes, many patients travel abroad for these procedures to access high-quality care at lower costs. Countries like Turkey, India, and Iran offer world-class cardiac centers facilitated by WMedTour.
What is the recovery time for TAVI?
TAVI recovery is swift. Most patients leave the hospital within 2 to 3 days. Full resumption of daily activities often occurs within a week or two, which is significantly faster than open surgery.
Does insurance cover TAVI procedures abroad?
It depends on your provider. Some international insurance plans cover treatments abroad. However, many medical tourists pay out-of-pocket because the cost is significantly lower than their deductible or local private rates.
Am I awake during the TAVI procedure?
Often, yes. TAVI can be performed under conscious sedation (twilight anesthesia). You are relaxed and feel no pain but are not fully unconscious like in general anesthesia used for open-heart surgery.
What are the risks of stroke in TAVI vs. SAVR?
When comparing TAVI (Transcatheter Aortic Valve Implantation) and SAVR (Surgical Aortic Valve Replacement), stroke remains one of the most critical risks discussed by Heart Teams.
In 2025, the data shows a complex relationship between the two procedures: TAVI often has a slight advantage in the immediate 30 days, but surgery may have a slight advantage in long-term stroke prevention.
1. Early Risk (The First 30 Days)
TAVI Advantage: TAVI typically shows a lower risk of immediate stroke compared to open-heart surgery. This is because surgery involves a heart-lung machine and more invasive manipulation of the aorta, which can dislodge calcium or tissue.
The Difference: In many clinical trials, the rate of disabling stroke within 30 days is roughly 1.0% for TAVI versus 2.5% for SAVR.
2. Mid-to-Long-Term Risk (1–5 Years)
The “Catch-Up” Effect: Research suggests that while TAVI starts safer, the stroke risk curves eventually meet or even flip.
SAVR Advantage: Beyond the two-year mark, some studies show a slightly higher stroke rate in TAVI patients. This may be due to “subclinical leaflet thrombosis”—small blood clots that can form on TAVI valve leaflets—which are less common in surgical valves.
3. Disabling vs. Non-Disabling Strokes
Severity: Doctors distinguish between a “disabling stroke” (permanent impact on daily life) and a “non-disabling stroke.”
Consensus: For most low-risk patients, the 5-year rate of disabling stroke is remarkably similar between the two procedures (around 3.5% to 4%).
4. Cerebral Protection Devices
To make TAVI even safer, surgeons often use Cerebral Embolic Protection (CEP) devices.
What they do: These act like a “net” in the arteries leading to the brain to catch debris during the procedure.
Update: Recent large-scale trials have shown that while these devices are safe, they don’t significantly reduce the overall stroke rate for every patient. However, they are still recommended for patients with heavily calcified valves who are at high risk.
Risk Comparison Summary
| Timeline | TAVI Stroke Risk | SAVR Stroke Risk | Winner |
| 0–30 Days | Lower (~1%) | Higher (~2.5%) | TAVI |
| 1 Year | Comparable | Comparable | Tie |
| 5 Years | Slightly Higher | Slightly Lower | SAVR |
Can a TAVI valve be replaced if it fails?
Here is the updated content regarding TAVI valve replacement, with all citations and source markers removed:
Yes, a TAVI valve can be replaced if it fails, but the approach is different from a traditional surgical replacement. In 2025, doctors primarily use a technique called Valve-in-Valve (ViV).
Here is the breakdown of how a failing TAVI valve is managed and what you need to know about the future of your heart health:
1. The Valve-in-Valve (ViV) Procedure
If your TAVI valve wears out or begins to leak after several years, specialists can often perform a second TAVI.
How it works: A new, collapsible TAVI valve is guided via catheter into the center of the old, failing TAVI valve.
The Result: The new valve expands, pushing the old one against the heart wall and taking over the job of regulating blood flow.
Benefit: This avoids the need for open-heart surgery, which is especially beneficial for older patients who may be more frail than they were during their first procedure.
2. Surgical “Explant” (The Complex Option)
If a Valve-in-Valve procedure is not possible—perhaps due to the risk of blocking blood flow to the coronary arteries—the old TAVI valve must be surgically removed.
The Challenge: Unlike a surgical valve, which is sewn in with thread, TAVI valves use a metal frame that “nests” into your heart tissue. Over time, your body grows tissue around this frame.
The Risk: Removing a TAVI valve is a highly complex surgery that carries more risk than a standard first-time heart surgery. This is why surgeons often prefer surgery for younger patients initially; it leaves a “cleaner” environment for future treatments.
3. Lifetime Management Planning
Because we can now replace valves within valves, cardiologists use the term “Lifetime Management.”
First Intervention: If you start with a surgical valve, you can usually have a TAVI inside it later (TAVI-in-SAVR).
Second Intervention: If you start with TAVI, you might be able to do another TAVI (TAVI-in-TAVI).
Factors That Determine If Your Valve Can Be Replaced:
Anatomy: Is there enough room for a second valve without blocking the arteries that feed the heart?
Valve Size: Was the first valve large enough? Small valves are harder to “double up.”
Reason for Failure: Is the valve just worn out (calcified), or is there an infection (endocarditis)? Infections almost always require surgery rather than a second TAVI.
Why is TAVI more expensive in some countries?
The TAVI valve device itself is technologically advanced and expensive to manufacture. While hospital stays are shorter, the high cost of the device can make the total procedure price high in Western countries compared to medical tourism destinations.
Who decides which surgery is best for me?
In modern cardiac care, the decision is not made by a single person. Instead, it is made by a specialized group of experts known as the Heart Team.
This collaborative approach ensures that you receive a recommendation based on multiple perspectives rather than a single surgeon’s or cardiologist’s preference.1
👥 Members of the Heart Team
The team typically includes:
Interventional Cardiologist: A specialist who performs TAVI and other catheter-based procedures.2
Cardiac Surgeon: A specialist who performs traditional open-heart surgery (SAVR).
Imaging Specialist: A doctor (often a radiologist or cardiologist) who interprets your CT scans and echocardiograms to check your heart’s anatomy.3
Anesthesiologist: Evaluates your ability to handle general anesthesia or conscious sedation.
Clinical Coordinator: Often your main point of contact, ensuring all tests and consultations are organized.
📋 How They Make the Decision
The Heart Team reviews your case based on three main pillars:
Surgical Risk (STS Score): They use a standardized scoring system to calculate the statistical risk of surgery based on your age, lung function, kidney health, and previous surgeries.
Anatomy: They look at the size of your arteries (to see if a TAVI catheter can pass) and the shape of your valve (to see if a replacement will sit securely).
Lifestyle and Life Expectancy: They consider how active you are and how many years you need the valve to last. For a patient who is 85, TAVI is often the clear winner. For a healthy 60-year-old, surgery is usually favored.
🗣️ Your Role in the Decision
While the Heart Team provides the clinical recommendation, you (the patient) have the final say. Shared Decision-Making (SDM) is the gold standard for 2025. This means the team should explain the pros and cons of both options clearly to you and your family, allowing you to choose the path that aligns with your personal values—whether that is “the fastest possible recovery” or “the most durable long-term solution.”
Is open-heart surgery better for younger patients?
In 2025, the medical consensus generally favors Open-Heart Surgery (SAVR) for younger patients (typically those under 65 or 75, depending on the region), primarily due to concerns over valve durability and lifetime management.
While TAVI (Transcatheter Aortic Valve Implantation) is gaining popularity for its fast recovery, clinical evidence and 2025 guidelines highlight several reasons why surgery remains the “gold standard” for younger populations:
1. Superior Long-Term Durability
Younger patients have a longer life expectancy, often needing their replacement valve to last 20 years or more.1
The Durability Gap: Current data suggests that surgical bioprosthetic valves have a more established track record for long-term durability. Recent studies (2024–2025) indicate that TAVI valves may show higher rates of structural deterioration or “hemodynamic decline” after the 5-to-8-year mark compared to surgical ones.
Reintervention Risk: If a TAVI valve fails in a young patient, a second procedure (TAVI-in-TAVI or a complex surgical “explant”) is required. Recent data shows that removing a TAVI valve surgically is much more dangerous than a standard re-operation.
2. Lower Rates of Pacemakers & Leaks
Pacemakers: TAVI has a significantly higher risk of disrupting the heart’s electrical system. Younger patients undergoing TAVI are nearly 3 times more likely to need a permanent pacemaker compared to those having surgery.2
Paravalvular Leak (PVL): Small leaks around the edge of the valve are more common with TAVI. While these might be tolerable for an 85-year-old, even a mild leak can cause heart strain over 20+ years in a younger person.
3. Anatomical Advantages (Bicuspid Valves)
Many younger patients have a Bicuspid Aortic Valve (a birth defect where the valve has two leaflets instead of three).
Surgery is almost always preferred for bicuspid valves because TAVI devices struggle to fit perfectly in these asymmetrical openings, leading to higher failure rates.
Comparison Summary for Younger Patients
| Feature | Open-Heart Surgery (SAVR) | TAVI (Transcatheter) |
| Primary Goal | Lifetime durability (20+ years) | Quick recovery & low trauma |
| Guideline Status | Recommended for patients <65 | Recommended for patients >75 |
| Valve Lifespan | Very high (especially mechanical) | Still being studied beyond 10 years |
| Pacemaker Risk | Low (~3–5%) | Higher (~15–20%) |
| Recovery | 2–3 months | 1–2 weeks |
The “Heart Team” Decision
The 2025 ESC/AHA guidelines stress that for patients between 65 and 75, the choice is not “one size fits all.” It requires a Heart Team discussion that weighs your specific anatomy, lifestyle, and how many heart procedures you might reasonably face in your lifetime.
Medical Disclaimer: The information provided in this blog post is for educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional or cardiologist for diagnosis and treatment of any heart condition. WMedTour does not provide medical services directly but facilitates connections with accredited medical providers.
References:
American Heart Association
European Society of Cardiology