👁️ Why Some Surgeons Still Perform ICCE Cataract Surgery
📄 Executive Summary
Many patients today wonder why surgeons would still use an older technique like ICCE (Intracapsular Cataract Extraction), given modern alternatives. While ICCE has largely been replaced by safer methods like Phaco and ECCE, top eye surgeons still choose ICCE in rare and specific situations. This guide explains exactly when and why ICCE is performed, the risks and benefits, how it compares with other surgeries, and what international patients should consider when exploring cataract surgery abroad.
🧠 What Is ICCE Cataract Surgery?
Intracapsular Cataract Extraction (ICCE) is a surgical technique in which the entire natural lens and its surrounding capsule are removed in one piece. This differs from modern methods where only the cloudy lens is removed and the capsule is left intact to support an intraocular lens implant. ICCE requires a large incision and traditionally had higher complication rates compared to newer techniques. ICCE remains rare today but continues in exceptional clinical cases worldwide.
How ICCE Works
- Surgeon creates a large incision in the eye
- Entire lens and lens capsule removed together
- Often followed by lens replacement in a secondary location
📉 Why ICCE Fell Out of Favor
ICCE once served as a mainstream cataract solution, but improved surgical tools and modern techniques like ECCE (Extracapsular Cataract Extraction) and Phacoemulsification significantly reduced risks and improved vision outcomes. ECCE preserves the capsule, allowing a stable intraocular lens (IOL). Phaco uses ultrasonic energy to break the lens into tiny pieces, allowing very small incisions and rapid healing. ICCE declined primarily because it exposed the eye to greater complications.
🔍 Why Some Surgeons Still Perform ICCE Today
Despite being considered outdated in most settings, surgeons still perform ICCE in carefully selected cases. These include conditions where modern techniques are unsafe or unfeasible. Below are the main reasons ICCE remains in practice:
1. Severe Zonular Weakness or Subluxation
When the fibers (zonules) that normally hold the lens in place are extremely weak or broken, surgeons may not be able to preserve the capsule. In these cases, ICCE may be the safest option to fully remove the damaged lens.
2. Traumatic Eye Injuries
In eyes with a history of severe trauma, the lens may be dislocated or destabilized. Surgeons may choose ICCE because other methods risk more harm.
3. Lack of Advanced Equipment
In remote or under‑resourced medical settings where advanced microscopes or phacoemulsification equipment are unavailable, experienced surgeons sometimes use ICCE rather than delaying treatment. {index=4}
4. Specialized Clinical Scenarios
Certain rare genetic or pathological conditions make preserving the capsule dangerous or impossible. In these cases, well‑trained surgeons may still perform ICCE.
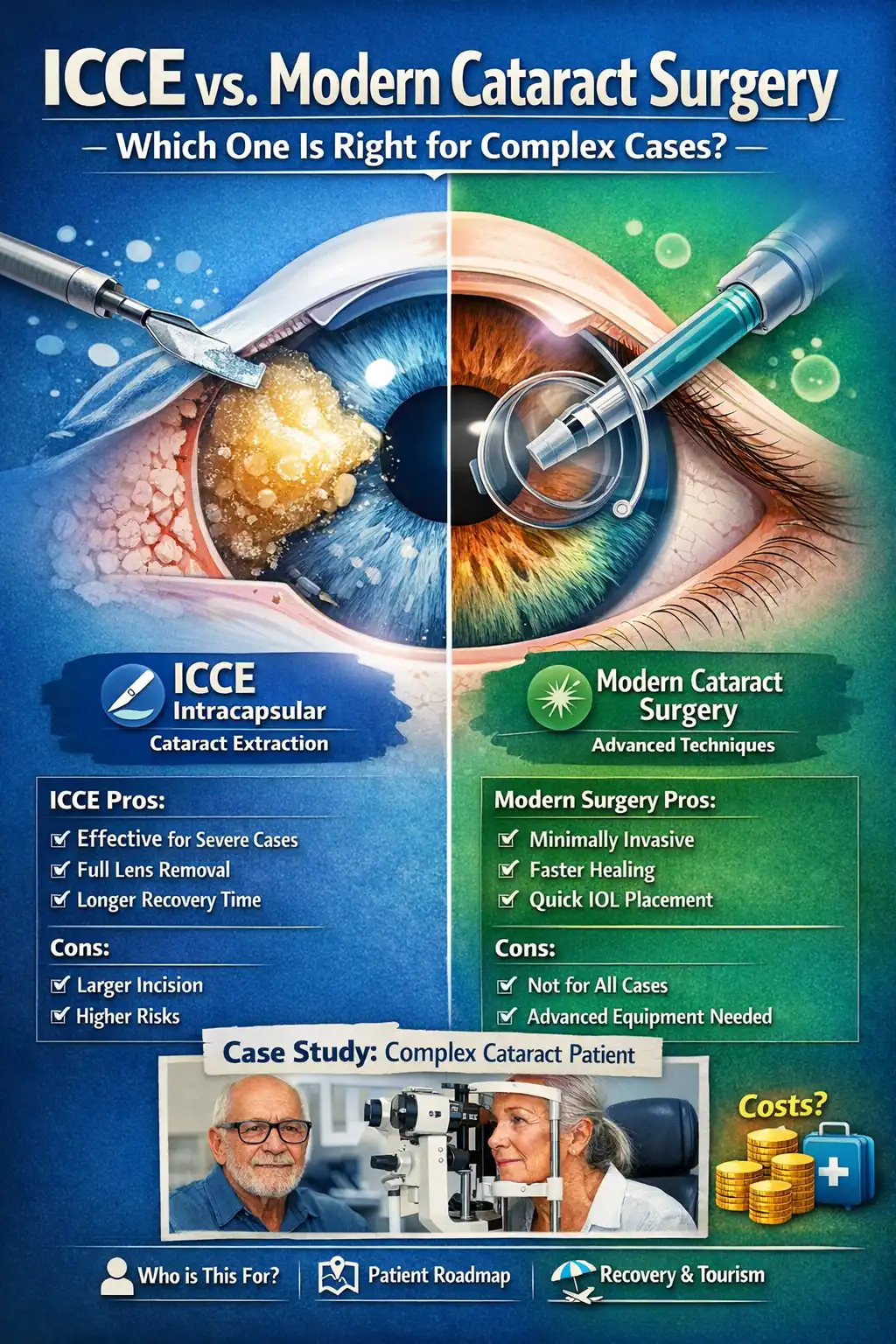
⚖️ ICCE vs Modern Alternatives: Pros and Cons
| Aspect | ICCE | Modern Techniques (Phaco/ECCE) |
|---|---|---|
| Incision Size | Large (≈10–12 mm) | Tiny (≈2–3 mm) |
| Capsule Preservation | No | Yes |
| Complication Risk | Higher | Lower |
| Recovery Time | Longer | Faster |
| Use in Complex Cases | Sometimes necessary | Often unsuitable if capsular support is lost |
👤 Who Is This For?
- Patients with uncommon eye conditions requiring specialized surgical decisions.
- Medical tourists researching advanced or rare cataract surgery options abroad.
- Eye care professionals who need a deeper understanding of rare surgical indications.
- Individuals seeking to balance safety, costs, and surgical outcomes globally.
🛣️ Patient Roadmap: From Consultation to Recovery
Step 1: Pre‑Surgery Evaluation
Your surgeon will perform a full eye exam, including ultrasound and retina checks to assess lens position and capsule integrity. They may recommend ICCE only when preserving the capsule is unsafe.
Step 2: Choosing a Destination
Medical tourists should consider factors like surgeon experience, technology availability, and cost. Options often include travel to centres in Iran, Oman, or India.
Step 3: Surgery Day
ICCE typically takes longer than a modern phacoemulsification procedure due to the larger incision and careful removal of the entire capsule.
Step 4: Recovery & Follow‑Up
Recovery is slower, often spanning several weeks. Regular follow‑up visits help monitor vision and prevent complications. Post‑op care may include in‑person and virtual check‑ins through telemedicine consultation.
💰 Cost Analysis Table (Estimates for ICCE vs Modern Surgery)
| Country | ICCE Cost | Phaco / ECCE Cost | Notes |
|---|---|---|---|
| Iran | $1,500 – $2,000 | $1,800 – $2,500 | Experienced surgeons, competitive pricing |
| India | $1,200 – $1,800 | $1,500 – $2,200 | High volume surgical centres |
| Oman | $1,700 – $2,500 | $2,000 – $3,000 | Premium care, higher living costs |
🧘 Recovery & Medical Tourism Tips
Unlike phaco, ICCE patients may need longer stays after surgery. Allow at least 2–4 weeks in your destination to ensure proper monitoring and follow‑up. Gentle activities and avoiding dusty or strenuous conditions are recommended throughout recovery.
📊 Case Study: A Complex Zonular Weakness Patient
Maria, age 68, presented with severe zonular instability following trauma. Ultrasound showed an unstable capsule. After careful evaluation by our surgeons in Iran, ICCE was chosen. The surgery restored her vision. Recovery took four weeks, and she enjoyed supervised leisure tourism while receiving post‑op care.
❓ FAQs – Understanding ICCE Indications
Why do some surgeons still perform ICCE?
Surgeons use ICCE when modern techniques cannot preserve the lens capsule safely due to trauma or zonular instability.
Is ICCE more risky than other cataract surgeries?
Yes — ICCE (Intracapsular Cataract Extraction) is significantly more risky than modern cataract surgeries like ECCE or phacoemulsification. Here’s why:
🔹 Why ICCE Is Riskier
- Capsule Removal
- ICCE removes the entire lens including the capsule, which normally provides support for the intraocular lens (IOL).
- Loss of the capsule increases the risk of lens instability, retinal detachment, and vitreous complications.
- Large Incision
- Requires a much bigger wound than modern surgeries.
- Larger incision → more trauma, higher infection risk, longer healing, and more astigmatism.
- Vitreous Loss
- Without the capsule, the vitreous body can prolapse, leading to complications such as retinal tears or macular edema.
- Slower Visual Recovery
- Healing takes longer due to the large incision and increased inflammation.
- IOL Complications
- Lens must be placed in the anterior chamber or sutured, which is less stable than capsule-supported IOLs used in ECCE or phaco.
🔹 Comparison of Risks
| Surgery Type | Capsule Preserved? | Incision Size | Complications | Recovery |
|---|---|---|---|---|
| ICCE | No | Very Large | High (retinal detachment, vitreous loss, infection, astigmatism) | Slow |
| ECCE | Yes | Large | Moderate (corneal edema, astigmatism, less retinal risk) | Moderate |
| Phaco | Yes | Tiny | Low (rare infection, minimal astigmatism) | Fast |
✅ Key Takeaway
- ICCE is the most risky cataract surgery, largely replaced by modern ECCE and phaco because they are safer, faster, and more predictable.
- ICCE is only used today for extremely complex eyes where the capsule is destroyed or the lens is fully dislocated.
Can ICCE be done anywhere?
No — ICCE (Intracapsular Cataract Extraction) cannot be done just anywhere today.
Here’s why:
🔹 Why ICCE Is Limited
- Specialized Indications
- ICCE is only performed when the lens capsule cannot be preserved, or the lens is severely dislocated.
- Most eyes are suitable for phacoemulsification or ECCE, which are safer and more predictable.
- Declining Expertise
- Modern surgeons are trained primarily in phaco and ECCE.
- Few surgeons today have routine experience with ICCE, making it rare in standard ophthalmic centers.
- High-Risk Procedure
- ICCE has a higher risk of complications: retinal detachment, vitreous loss, astigmatism, and infection.
- Hospitals must have advanced surgical support and emergency vitreoretinal backup to manage complications safely.
- Resource Requirements
- Although ICCE requires less modern equipment than phaco, it still needs a fully equipped operating room, skilled anesthetic support, and post-op monitoring.
🔹 Realistic Availability
- Mostly in specialized or trauma centers, often in developing countries or cases where modern surgery is impossible.
- Not offered routinely in hospitals that cater to international patients or standard cataract care.
- For international patients, phacoemulsification or ECCE is almost always the option.
✅ Key Takeaway
- ICCE cannot be done everywhere — it’s a rare, last-resort procedure performed only in select centers with surgeons experienced in complex, high-risk cataract cases.
Does ICCE require a longer recovery?
Yes — ICCE requires a significantly longer recovery than modern cataract surgeries like ECCE or phacoemulsification. Here’s why:
🔹 Reasons Recovery Is Longer After ICCE
- Large Incision
- ICCE uses a very large surgical incision (often 10–12 mm or more) compared to tiny phaco incisions.
- Larger wounds take weeks to months to fully heal and may require sutures, increasing recovery time.
- Capsule Removed
- The entire lens capsule is removed, so the IOL is placed in the anterior chamber or sutured, which can take additional time to stabilize.
- Higher Post-Op Inflammation
- More tissue trauma → swelling, discomfort, and inflammation that slow vision recovery.
- Astigmatism and Visual Correction
- Large incisions can induce significant astigmatism, meaning glasses may be needed longer, further extending the adjustment period.
- Risk of Complications
- Higher rates of retinal detachment, vitreous loss, and corneal issues mean that careful monitoring and slower recovery are required.
🔹 Typical Recovery Timelines
| Surgery Type | Initial Visual Improvement | Full Recovery / Stabilization |
|---|---|---|
| ICCE | Several days to 1 week | 4–8+ weeks, sometimes months |
| ECCE | 1–3 days | 2–6 weeks |
| Phaco | 1–2 days | 1–4 weeks |
✅ Key Takeaway
- ICCE has the slowest recovery of all cataract surgeries.
- Modern techniques like phaco offer faster healing, less inflammation, and quicker visual stabilization, making them the preferred choice for most patients, including complex eyes.
Are intraocular lenses used after ICCE?
Yes — intraocular lenses (IOLs) are used after ICCE, but the approach is different from modern cataract surgery because the lens capsule is removed. Here’s how it works:
🔹 IOL Placement After ICCE
- No capsule support
- Unlike phaco or ECCE, ICCE removes the entire lens and its capsule.
- Normally, IOLs are placed inside the capsule, but that’s not possible here.
- Alternative IOL Options
- Anterior chamber IOL (ACIOL):
- Placed in the front part of the eye (between the cornea and iris).
- Requires proper sizing and careful placement to avoid complications.
- Scleral-fixated or sutured posterior IOL:
- Secured to the sclera (white of the eye) or iris.
- More technically demanding and requires a highly skilled surgeon.
- Anterior chamber IOL (ACIOL):
- Visual Outcomes
- IOL placement after ICCE can restore vision, but:
- Stability may be less predictable than capsule-supported IOLs.
- Risk of complications is higher (dislocation, glaucoma, corneal issues).
- IOL placement after ICCE can restore vision, but:
🔹 Comparison With Modern Surgery
| Feature | ICCE | ECCE / Phaco |
|---|---|---|
| Capsule | Removed | Preserved |
| IOL placement | Anterior chamber or scleral-fixated | In the capsule (stable) |
| Complication risk | Higher (IOL dislocation, glaucoma) | Lower |
| Recovery & vision stabilization | Slower | Faster and more predictable |
✅ Key Takeaways
- IOLs are used after ICCE, but require alternative fixation techniques because the capsule is gone.
- Modern cataract surgery (ECCE or phaco) is preferred because capsule-supported IOLs are safer, more stable, and lead to faster visual recovery.
Can ICCE be combined with other eye procedures?
Yes — ICCE can sometimes be combined with other eye procedures, but it’s less common than with modern cataract surgery due to its higher risk and complexity. Here’s a detailed explanation:
🔹 Possible Combinations
- Vitrectomy (removal of vitreous gel)
- Often performed if the lens is dislocated or there’s trauma.
- ICCE may be done together with pars plana vitrectomy to safely remove the lens and stabilize the eye.
- Corneal Procedures
- Rarely, ICCE may be combined with corneal transplant or repair in eyes with significant trauma or corneal disease.
- Glaucoma Surgery
- Can be combined with procedures like trabeculectomy, but careful planning is required because ICCE increases post-op inflammation and risk.
- Retinal Procedures
- ICCE may be combined with retinal detachment repair if lens removal is needed to access the vitreous or retina.
🔹 Limitations
- High complication risk makes combining ICCE with other procedures more challenging.
- Longer surgical time → higher risk of bleeding, inflammation, or infection.
- Only experienced surgeons in specialized centers perform these combined procedures.
🔹 Comparison With Modern Surgery
| Feature | ICCE | ECCE / Phaco |
|---|---|---|
| Can combine with vitrectomy | Yes, but high risk | Yes, safer and more common |
| Can combine with corneal / glaucoma procedures | Rare | More common, safer |
| Surgical complexity | Very high | Moderate |
| Recovery | Long | Faster |
✅ Key Takeaways
- ICCE can be combined with other eye procedures, but only in complex, high-risk cases.
- Modern surgeries (ECCE or phaco) are much safer and more flexible for combining with glaucoma, corneal, or retinal procedures.
Is ICCE cheaper than modern surgery?
Yes — ICCE is generally cheaper upfront than modern cataract surgery (phacoemulsification or ECCE), but there are important nuances.
🔹 Why ICCE May Cost Less Initially
- Minimal equipment needed
- ICCE is largely manual and does not require advanced phaco machines or lasers.
- Fewer disposable instruments → lower surgical cost.
- Shorter operating room setup
- Simpler instruments and no sophisticated machines → reduced facility fees.
🔹 Why True Cost May Be Higher
- Higher complication risk
- ICCE carries more risk of retinal detachment, vitreous loss, infection, and IOL issues.
- Managing complications may require additional surgeries, longer follow-up, or medications, which can increase overall cost.
- Longer recovery
- More post-op care, follow-up visits, and slower return to work or daily activities → indirect costs may be higher.
- IOL considerations
- ICCE requires anterior chamber or sutured IOLs, which may be more expensive or technically demanding in some centers.
🔹 Cost Comparison Overview
| Surgery Type | Equipment Needs | Upfront Cost | Overall Value / Risk |
|---|---|---|---|
| ICCE | Minimal | Low | Higher risk → may increase total cost |
| ECCE | Moderate | Moderate | Safer than ICCE, moderate recovery |
| Phaco | Advanced | Higher | Lower risk, faster recovery, often better long-term value |
✅ Key Takeaways
- ICCE can appear cheaper initially, but the high complication risk and longer recovery may make it less cost-effective overall.
- Modern phacoemulsification is slightly more expensive upfront but offers faster recovery, fewer complications, and more predictable outcomes, making it the preferred choice for most patients, including international ones.
Who is NOT a candidate for ICCE?
Not everyone is a candidate for ICCE (Intracapsular Cataract Extraction). In fact, most patients today are not suitable, because ICCE is a high-risk, last-resort procedure. Here’s a clear breakdown:
🔹 Who Is NOT a Candidate for ICCE
- Patients with intact lens capsule
- ICCE removes the capsule, so if the capsule is healthy, modern phaco or ECCE is safer and preferred.
- Patients with normal or mildly complex eyes
- Simple age-related cataracts do not require ICCE; safer, faster surgeries exist.
- Patients at high risk for post-op complications
- Examples: uncontrolled glaucoma, severe corneal disease, retinal disorders.
- ICCE increases risk of retinal detachment, vitreous loss, and corneal issues.
- Patients seeking fast recovery
- ICCE has a slower recovery and more post-op discomfort; anyone needing quick visual restoration (e.g., travelers, working patients) is better off with phaco.
- International patients or medical tourists
- Most centers that treat international patients do not perform ICCE routinely due to high risk and specialized surgical expertise required.
- Patients unwilling or unable to follow strict post-op care
- ICCE requires longer follow-up, frequent monitoring, and careful management of complications.
🔹 Key Takeaways
- ICCE is reserved only for extremely complex eyes, such as:
- Lens completely dislocated into the vitreous
- Capsule destroyed due to trauma or previous surgery
- Most cataract patients are NOT candidates — phaco or ECCE is almost always preferred.
Is ICCE still taught in ophthalmology training?
In some regions, surgeons train with ICCE for rare cases.
How long does ICCE surgery take?
More time than modern methods due to complexity and incision size.
What are alternatives if ICCE isn’t suitable?
If ICCE (Intracapsular Cataract Extraction) isn’t suitable, there are safer, more effective alternatives that are used in nearly all modern cataract surgeries. Here’s a detailed overview:
🔹 Primary Alternatives to ICCE
1. Phacoemulsification (Phaco)
- How it works: Ultrasound breaks up the lens, which is removed through a tiny incision. Capsule is preserved.
- Advantages:
- Fast recovery (1–4 weeks)
- Minimal astigmatism
- Safer and lower complication risk
- Capsule-supported IOL placement for stable vision
- Best for: Most cataract patients, including complex eyes with modern surgical tools.
2. Extracapsular Cataract Extraction (ECCE)
- How it works: The lens nucleus and cortex are removed, but the posterior capsule is preserved. Larger incision than phaco.
- Advantages:
- Capsule preserved → standard IOL implantation
- Can handle very dense or advanced cataracts that phaco may struggle with
- Best for: Hard cataracts, eyes with zonular weakness, or where phaco equipment isn’t available.
3. Manual Small Incision Cataract Surgery (MSICS)
- How it works: A self-sealing, moderately sized incision is made to remove the lens manually. Capsule preserved.
- Advantages:
- Less technology-dependent than phaco
- Faster and safer than ICCE
- Good option in resource-limited settings
- Best for: Dense cataracts in regions without phaco machines.
4. Laser-Assisted Cataract Surgery (Femtosecond Laser)
- How it works: Laser is used to make corneal incisions, open the capsule, and pre-soften the lens before phaco removal.
- Advantages:
- High precision
- Safer in complex eyes
- Reduces ultrasound energy needed → less corneal stress
- Best for: Patients seeking high precision and minimal complications, often combined with phaco.
🔹 Why These Are Preferred Over ICCE
| Feature | ICCE | Modern Alternatives (Phaco / ECCE / MSICS / Laser) |
|---|---|---|
| Capsule preserved? | No | Yes (stable IOL placement) |
| Incision size | Very large | Tiny (Phaco), Moderate (ECCE/MSICS) |
| Complication risk | High | Low to moderate |
| Recovery | Long | Fast to moderate |
| Visual outcome | Less predictable | Highly predictable |
✅ Key Takeaways
- ICCE is rarely needed today — only in extreme cases (trauma, destroyed capsule, fully dislocated lens).
- Modern cataract surgeries (phaco, ECCE, MSICS, laser-assisted) are safer, faster, and give better visual outcomes.
- Surgeons typically choose these alternatives even in complex or international patient cases.
Can international patients find ICCE abroad?
Technically, yes — ICCE (Intracapsular Cataract Extraction) is still performed in some parts of the world, but for international patients it’s extremely rare. Here’s why:
🔹 Availability of ICCE Abroad
- Very few centers perform ICCE today
- Modern phacoemulsification and ECCE have almost entirely replaced ICCE because they are safer, faster, and have better visual outcomes.
- Situations where ICCE might be offered
- Severe trauma or completely dislocated lens
- Extremely fragile or destroyed lens capsule
- Rare cases where modern equipment or techniques fail or are unavailable
- International patient perspective
- Most hospitals catering to medical tourists do not offer ICCE, because it carries higher complication rates and slower recovery.
- If ICCE is performed, it’s usually in low-resource or specialized trauma centers, not standard medical tourism clinics.
🔹 Key Takeaways
- ICCE is largely historical — it’s a last-resort technique, not a first choice.
- International patients seeking cataract surgery are almost always offered phacoemulsification or ECCE instead.
- If ICCE is considered, it’s usually because the eye has extreme damage or complications making modern surgery unsafe.
In short: for most international patients, ICCE is not realistically available abroad, and even if it is, it is only done for very specific, high-risk cases.
⚠️ Medical Disclaimer
This post is for educational purposes only. ICCE and other cataract surgeries carry risks. Consult a qualified ophthalmologist before making any medical decisions.
🌐 Explore More